



Workshop with Médecins Sans Frontières: Experiences and Lessons Learned from Humanitarian Action in Sudan, March 2026

On 25 March 2026, a group of students enrolled in the Bachelor's Degree Programme in Political Science, International Relations and Human Rights at the University of Padua took part in an intensive workshop organised by Médecins Sans Frontières (MSF) Italy on humanitarian action in Sudan.
Since 1971, Médecins Sans Frontières has been committed to providing medical and humanitarian assistance wherever access to healthcare is denied. The organisation originated during the Biafran War in Nigeria, when a group of French Red Cross doctors, deeply shaken by the atrocities of the genocide and frustrated by the obligation to remain silent, decided to speak out.
At the same time, several journalists returning from an emergency mission in Bangladesh shared the same urgent need to bear witness. Raymond Borel and Philippe Bernina, journalists at the medical journal Tonus, consequently launched an appeal to establish a team of relief workers ready to respond to the world's most severe disasters. MSF was officially founded on 22 December 1971 by 300 volunteers. The success of its early missions, including those in Nicaragua and Managua, and its unwavering commitment to its mission led to the organisation being awarded the Nobel Peace Prize in 1999.
The workshop began with a presentation by Dr Sara Lina Kamoun on international humanitarian law (IHL). IHL regulates the conduct of hostilities, protects those who are not directly participating in the fighting, and restricts the means and methods of warfare. Its sources include the 1949 Geneva Conventions, their Additional Protocols, and customary international law. The primary purpose of this body of law is to protect civilians, medical personnel, and relief operations, and it is binding on both state and non-state actors. IHL applies strictly to international and non-international armed conflicts, but not to situations involving internal tensions alone.
Dr Kamoun then introduced the core humanitarian principles of humanity, neutrality, impartiality, and independence. Humanity requires suffering to be addressed wherever it is found, with the aim of protecting life and ensuring respect for human beings. Neutrality requires humanitarian actors to refrain from taking part in hostilities or becoming involved in controversies of a political, racial, or religious nature. Impartiality means that action must be guided solely by need, prioritising the most urgent cases without distinction as to nationality or belief. Finally, independence ensures that humanitarian action remains autonomous from political, economic, or military objectives.
The discussion then turned to the application of these principles in complex emergencies, where conditions on the ground create continual operational dilemmas. One of the main challenges is balancing staff safety with the principle of humanity and negotiating access without compromising neutrality, particularly when neutral actors risk being perceived as taking sides because of their language, behaviour, or symbols. In critical contexts, impartiality is tested by physical constraints on access, neutrality by donor conditions, and independence by host-state regulations.
In this setting, humanitarian principles emerge not as rhetorical formulas, but as strategic tools for strengthening credibility and legitimacy in negotiations. The work of Médecins Sans Frontières is therefore guided by these values together with the central principle of témoignage, or bearing witness: the duty to speak publicly about human rights violations while maintaining high standards of transparency and accountability towards patients and donors.
The transition from legal theory to operational reality lies at the heart of humanitarian action. It is not enough simply to know the rules; it is essential to understand how they can become practical tools. The connection between legal obligations and negotiation can be seen in the concept of protected status: knowing that medical personnel enjoy special protection is of little use unless this knowledge is translated into a credible negotiating strategy.
The proposed approach is to retain the Geneva Conventions as an ethical foundation without imposing them dogmatically, while prioritising negotiation in the field. This room for manoeuvre is constrained by the factors that shape the humanitarian environment: access and security depend on mapping the relevant actors and adapting language to different interlocutors, from national leaders to local authorities. Effectiveness also depends on coordination through the cluster system and on local participation, in accordance with the "Do No Harm" approach, so as to prevent aid from generating new tensions.
The workshop also addressed modern challenges, such as the presence of private military and security companies to which states delegate armed activities, thereby creating legal grey areas. Neutrality was also examined through the challenges encountered by MSF in the Russia-Ukraine war, where the inability to operate equally on both sides is often the result of restrictions on access imposed by the authorities rather than a political choice.
Sudan was a central case study, illustrating an exceptionally severe crisis that nevertheless receives limited media coverage. Despite Sudan's adherence to the Geneva Conventions, international humanitarian law is systematically violated: hospitals and healthcare facilities are deliberately destroyed by both parties, while severe malnutrition affects millions of people. Limited international attention results in funding cuts and turns healthcare assistance into an object of political negotiation, as authorities obstruct relief operations for fear that they may strengthen the enemy. In such contexts, negotiating safe passage requires specialised skills, local knowledge, and the ability to maintain a constant balance between access to aid and staff safety.
The workshop highlighted the alarming fragility of the humanitarian protection regime, as civilians and hospitals increasingly become deliberate targets of parties to conflicts. Nevertheless, IHL remains MSF's only instrument for protecting vulnerable people. Even when attacks on hospitals are justified by the alleged presence of combatants, the principle of proportionality must prevail.
In preparation for the simulation, every team member, from the head of mission to those responsible for healthcare, security, and communications, had to assume their responsibilities knowingly. Decision-making under pressure requires the integration of legal compliance, logistical feasibility, and ethical consistency. Humanitarian negotiation demands resilience and the moral courage to recognise when compromise is appropriate and when it is necessary to stand firm. It is this transition from understanding legal rules to exercising operational judgement that turns a humanitarian worker into a leader capable of acting effectively in the most complex crises.
The final part of the workshop focused on four realistic operational dilemmas drawn from the Sudanese context. These cases illustrated the practical difficulties of humanitarian work in the field and the constant tension between principles, security, and access. For each case, participants were asked to decide what MSF should do by choosing among various operational options and reflecting on the principles of humanitarian action and law, including impartiality, neutrality, access, security, and advocacy.
The first case concerned the dilemma of war surgery in Al-Fashir. In a city under siege by the Rapid Support Forces (RSF) and facing an extremely high number of casualties, the state refuses to authorise surgical programmes because it fears that enemy combatants may return to the front after receiving treatment. The central issue is humanitarian access as a response to urgent medical needs, which must take precedence over political considerations. The proposed strategic approach was to:
- Not allow the authorities' initial refusal to bring action to a halt.
- Begin operating, where technically feasible, even in the absence of a perfect legal and regulatory framework.
- Simultaneously open negotiations to obtain subsequent official recognition of the intervention.
This practice reflects the historical experience of organisations such as Médecins Sans Frontières, which have often secured legal recognition of their field presence only after demonstrating the life-saving impact of their work.
The second dilemma addressed access to aid from Chad through the Adré crossing, which had been blocked by the Sudanese government on security grounds despite the high risk of famine in Darfur. Faced with an impasse at the United Nations, which prioritises respect for national sovereignty, the humanitarian strategy should neither consist of violating borders nor passively accepting the blockade. Instead, the proposed approach was to:
- Continue sustained advocacy and political pressure.
- Use international humanitarian law as the essential legal basis for demanding access.
- Develop communications tailored to specific interlocutors, particularly individual influential states, rather than addressing the UN system in general terms.
The third scenario focused on speaking out about systematic violence against Masalit patients in El Geneina. This case revealed the profound tension between the mission to bear witness and the need to preserve access to healthcare. An immediate public statement could result in the expulsion of staff, leaving the population without assistance. The proposed gradual approach was to:
- Begin with confidential, bilateral communications with the parties concerned.
- Base every allegation on robust medical evidence that has been verified and securely archived.
- Prioritise the protection of the operational presence, strategically assessing the timing and form of communications in order to minimise the risk of retaliation.
Finally, the case of the Zamzam displacement camp highlighted the dramatic challenge of managing security under siege. With half a million people affected by malnutrition and a constant influx of wounded patients, the organisation must decide whether to remain despite the increasing risks to staff. Balancing risk and continuity of care does not allow for static responses, but requires the organisation to:
- Conduct continuous and dynamic risk assessments, as conditions can change rapidly.
- Maintain its presence for as long as possible, adapting activities to the facility's actual capacity.
- Exert constant pressure on the belligerents to comply with international humanitarian law.
Each dilemma confirmed that humanitarian action is not merely a medical undertaking. It is also an exercise in operational judgement in which legal legitimacy and negotiating capacity are the principal tools available to protect the most vulnerable.
In the MSF workshop on humanitarian dilemmas, participants were not simply asked to identify a general solution to each scenario. They were required to place themselves in the position of three different MSF professionals, each with a specific role and distinct perspective. The aim was to understand how these three professionals might respond to the same problem in complementary, but potentially different, ways.
The first role was that of the Project Coordinator, who holds overall responsibility for MSF's field activities. Their main task is to ensure that the project operates in accordance with humanitarian principles and security requirements. The Project Coordinator analyses the political and humanitarian context, maintains relations with local authorities, the UN, and other actors, and, above all, conducts negotiations for humanitarian access. They also define operational strategies and security measures. In the dilemmas, this professional therefore considered the feasibility of the intervention, access, and operational risk management.
The second role was that of the Humanitarian Affairs Manager, who is responsible for advocacy and humanitarian analysis. Their role is to collect data, testimonies, and information from the field and turn them into analysis and advocacy strategies. They also work to protect patients, shape the organisation's humanitarian positioning, and maintain relations with authorities and civil society. In the dilemmas, this professional focused primarily on the needs of affected populations, the documentation of violations, and political and institutional advocacy strategies, seeking to draw attention to crises without compromising humanitarian principles.
The third role was that of the Field Communications Manager, who is responsible for MSF's public communications in the country. They manage media relations, produce informational content, coordinate press releases and digital strategies, and may also act as a spokesperson. In addition, they monitor media coverage and respond to reputational crises or disinformation. In the dilemmas, this professional assessed how, when, and in what language the organisation should communicate externally, balancing transparency and media impact with operational security.
For each dilemma examined during the workshop, the task was therefore not to find a single answer, but to adopt the perspectives of these three professionals and understand how each would respond to the same situation. The Project Coordinator would prioritise access and operational security; the Humanitarian Affairs Manager would focus on needs, evidence, and advocacy; and the Field Communications Manager would assess the communication and media consequences of each decision. This exercise revealed the complexity of humanitarian work, in which every decision results from balancing different but interconnected perspectives.
The table below compares two of the world's most influential humanitarian organisations: Médecins Sans Frontières and the Red Cross. Although both share the fundamental mission of protecting human life, they differ in their structure, methods, and role within the international humanitarian system. The first difference concerns their institutional nature.
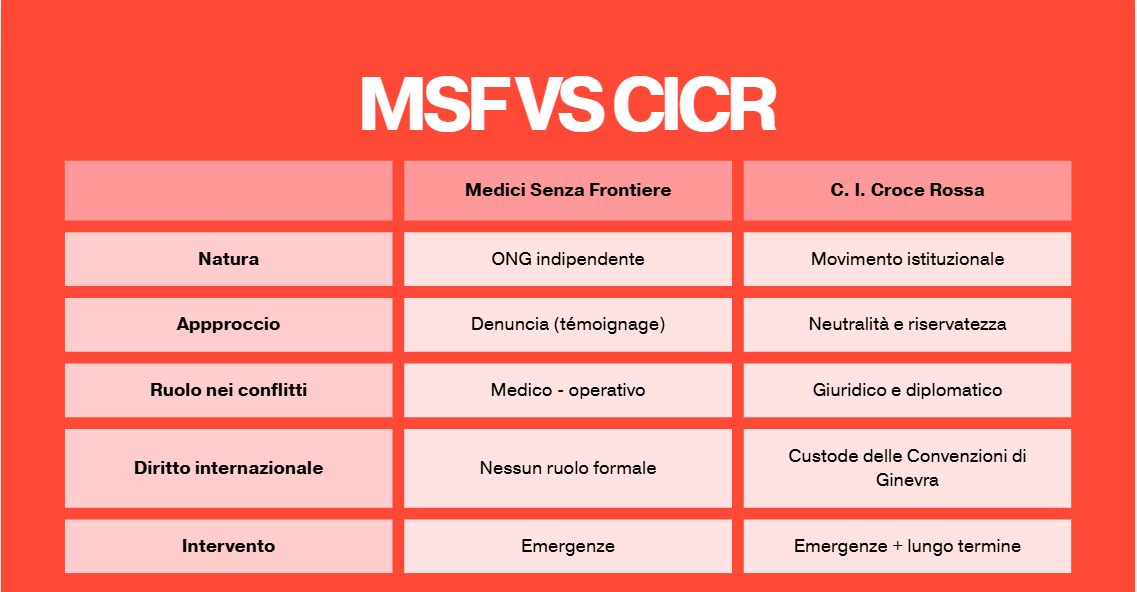
Médecins Sans Frontières is a fully independent non-governmental organisation, which enables it to intervene rapidly and without political constraints. In Sudan, for example, the authorities systematically obstruct humanitarian assistance for fear that it might strengthen the enemy, and only an organisation that is independent of state interests can continue operating in such a context.
The Red Cross, which is formally recognised by states, has a more institutionally constrained position. At the same time, this status gives it negotiating legitimacy and opens doors that might otherwise remain closed.
This distinction is reflected in their operational approaches. MSF combines medical action with the principle of témoignage: it publicly denounces human rights violations that it has witnessed directly, as in Sudan, where it has documented systematic attacks on healthcare facilities. The Red Cross, by contrast, adopts strategic neutrality, refraining from public statements in order to keep channels of dialogue open with all parties.
Their roles in armed conflicts also differ. MSF works directly in the field, providing emergency medical care. The Red Cross also operates at the legal and diplomatic levels: it acts as an intermediary between the parties and promotes compliance with international humanitarian law in its capacity as guardian of the Geneva Conventions. The treatment of prisoners of war offers a concrete example: visiting prisoners and verifying their conditions is a mandate entrusted specifically to the International Committee of the Red Cross and recognised by belligerents.
Finally, the two organisations operate across different time horizons. MSF prioritises rapid responses to acute emergencies, whereas the Red Cross combines immediate action with a long-term commitment, including the reconstruction of healthcare infrastructure after a conflict.
In essence, these two organisations are not alternatives, but complementary actors. MSF embodies rapid action and the courage to speak out, while the Red Cross provides continuity, dialogue, and institutional legitimacy. The interaction between these two models helps shape the architecture of global humanitarian action.